
Dr. Daniel Rivera, Plastic Surgery Resident II
Dr. Paola Uribe resident III dermatology
Seborrheic keratoses (SK) are the most common benign skin tumors in adults, however, their origin is not known with certainty. In SK, the epidermis is significantly replaced by basal cells without presenting malignant changes. The frequency is so high that it can be said that practically all senile adults have it. Their main clinical characteristic is that they are very well circumscribed and rounded in shape, with a warty and greasy surface that fissures easily. Their main characteristic on dermoscopic examination is the presence of keratin plugs or “horn pseudocysts”.
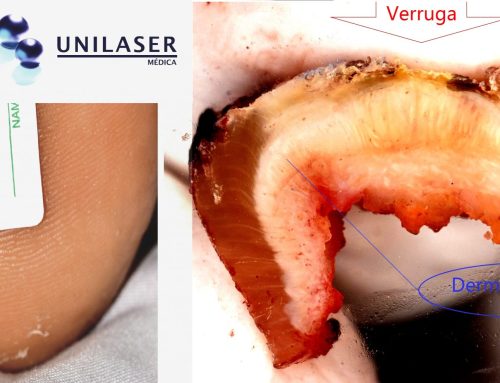
In the histological image, the epidermal ridges tend to elongate outwards, unlike the lentigines, which show a tendency towards the dermis.

The absence of QS in areas without hair follicles such as the palms and soles would seem to support its origin from the outermost portion of the hair follicle. Most QS have been shown to be monoclonal tumors, meaning they come from the same cell and do not have chromosomal abnormalities. An epidermal nevus will have a very similar clinical appearance but histology will show thickening of other cell lines such as the granular layer and an increase in the melanocytic line.
Mutations have been found in several genes such as PIK3CA and, importantly, FGFR3 , which is present in up to 85% of QS and has also been linked to the appearance of other tumors, including malignant tumors and more severe malformations such as craniosynostosis. However, the role in pathogenesis is still uncertain and no etiological factor has been identified.
There are different types of QS according to their microscopic structure. Each of the 9 types show different patterns of keratin and filaggrin (a protein that organizes keratin and helps keep the skin hydrated).
Laser has the advantage of treating smaller lesions. In larger lesions, all methods have shown the possibility of prolonged erythema, scarring and residual hypopigmentation. Compared to current techniques, laser is a new hope for trying to prevent these complications.

LITERATURE
Hafner, C., & Vogt,T. (2008). Seborrheic keratosis. Journal Der Deutschen DermatologischenGesellschaft , 6 (8), 664–677. http://doi.org/10.1111/j.1610-0387.2008.06788.x
31 – Tumors of the epidermis. (2015). 31 – Tumors of the epidermis. Weedon’s Skin Pathology (Fourth Edition, pp. 783–835.e29). Elsevier Ltd. http://doi.org/10.1016/B978-0-7020-5183-8.00031-X
Requena, L., Requena, C., & Cockerell, C.J. (2019). 109 – Benign epidermal proliferations and tumors. Dermatology ( Fourth Edition, pp. 1894–1916). Elsevier Espa8#241;a, SLU http://doi.org/10.1016/B978-84-9113-365-0/00109-1
Sanderson, K. V. (1968). The structure of seborrhoeic keratoses. The British Journal of Dermatology , 80 (9), 588–593.



{kind=link}
{kind=link}
{kind=link}
{kind=link}